![]()
Chapter 7: Improving the testing and management of syphilis
In this chapter
 Chapter 7 Download
Chapter 7 Download
Key points
- Notifications of infectious syphilis cases have risen significantly since 2012 with:
- an outbreak occurring among Aboriginal communities, predominantly affecting 15 to 29 year olds living in remote areas, with 15 to 19 year old women being the highest risk age group
- an increase among men who have sex with men (MSM), primarily living in urban areas.
- The re-emergence of congenital syphilis cases and deaths highlights the need to ensure prevention through increased antenatal screening, urgent management of affected women and their partners and improved engagement of pregnant and young women with health services.
- Practitioners should be familiar with the signs and symptoms of syphilis as well as the recent changes to the national syphilis testing and management guidelines, and maintain a low threshold for initiating treatment of cases and contacts.
- All health services and staff have an important role to play with regard to implementing the priority areas of the Enhanced response to addressing sexually transmissible infections (and blood borne viruses) in Indigenous populations action plan (National Syphilis Action Plan).
- The establishment of state and regional syphilis outbreak working groups has enabled effective communication and collaboration among government and non-government stakeholders to implement, monitor and evaluate the aims of the National Syphilis Action Plan.
- Syphilis point of care testing (POCT) is being rolled out in response to the syphilis outbreak and, while they have benefits, practitioners should be mindful of both the indications and limitations of their use.
Epidemiology
Syphilis has the potential to cause serious, but preventable, poor outcomes in pregnancy such as congenital syphilis as well as increasing the transmission of human immunodeficiency virus (HIV) and other sexually transmitted infections (STIs). Notifications of infectious syphilis cases in Australia increased significantly from 2012, with 4398 cases reported in 2017, indicating a doubling and tripling of cases among non-Indigenous and Aboriginal and Torres Strait Islander populations respectively. The differences in age and geographic distribution among the two main population groups most affected are as follows:
- an outbreak occurring among Aboriginal people, mainly affecting 15 to 29 year olds living in regional and remote areas in Western Australia (WA), Queensland (Qld), Northern Territory (NT) and South Australia (SA)
- increasing cases among MSM.
Among non-Indigenous people, 87 per cent of infectious syphilis cases have occurred among men, predominantly MSM living in major cities.
Current syphilis outbreak
Prior to the current outbreak, significant reductions in infectious syphilis had occurred among Aboriginal people living in remote areas with previously endemic levels of syphilis. Factors likely to have contributed to these reductions include the widespread use of antibiotics, effective syphilis screening programs and regionally based syphilis registers that have assisted with improved case detection and appropriate management. Despite those gains, an outbreak of infectious syphilis occurred recently, commencing in north-west Qld in 2011 and subsequently affecting communities in the NT, WA and SA, with more than 2344 cases notified.
In 2017, notification data of infectious syphilis cases among Aboriginal and Torres Strait Islander people identified the following:
- The majority of cases occurred among 15 to 29 year olds, similar to the age distribution of chlamydia and gonorrhoea notifications.
- 19 per cent of all notifications were among 15 to 19 year olds.
- 15 to 19 year old women are the highest risk age group.
- Cases are spread evenly between men and women.
- Remoteness is associated with increased notifications.
As of November 2018, seven confirmed cases of congenital syphilis and three deaths have been reported in the NT, Qld and SA.
Response to the syphilis outbreak
Responses to the syphilis outbreak have recognised the need for a multifaceted approach and to focus not just on syphilis but more broadly, to address the high rates of other STIs among populations affected. Responses have included the establishment of new strategies and strengthening of existing strategies including the:
- establishment of the Multijurisdictional Syphilis Outbreak Working Group (MJSO) by the Communicable Diseases Network of Australia (CDNA) in April 2015 to advise governments on coordinating the public health response for outbreak control and preventing transmission of syphilis from infected women to their babies, through rigorous antenatal testing and care
- development of the National Syphilis Action Plan by the Australian Health Protection Principal Committee (AHPPC) Governance Group and endorsed by the Australian Health Ministers' Advisory Council (AHMAC) in December 2017
- development of National Syphilis Guidelines by CDNA and updated in August 2018, to provide nationally consistent guidelines for public health units (PHUs) in responding to notifiable disease events
- development of public awareness raising campaigns such as ‘Young, Deadly, Syphilis Free' developed by the South Australian Health and Medical Research Institute (SAHMRI) and funded by the Australian government, which aims to:
- increase the uptake of testing for syphilis and other STIs among Aboriginal and Torres Strait Islander people aged 15 to 34 years
- test 30,000 young people in communities affected for syphilis and other STIs by June 2019.
The CDNA National Syphilis Action Plan and National Syphilis Guidelines have short and longer term goals that will be aligned with the Fifth National Aboriginal and Torres Strait Islander Blood-Borne Viruses and Sexually Transmissible Infections Strategy 2018–2022. Four priority areas identified in the action plan are:
- Testing and treatment: increasing the number of people tested, frequency of testing, the subsequent treatment of those infected and contact tracing of known sexual contacts
- Surveillance and reporting: enhancing the quality and improving access to laboratory testing data and development of key reporting indicators to monitor the outbreak.
- Education and awareness: access to consistent and appropriate resources for at-risk communities with a particular emphasis on young and pregnant women and the health workforce servicing these areas
- Antenatal care: ensuring consistent recommendations for repeat testing during pregnancy among women at high risk of infection and improving the management of perinatal syphilis.
In addition to the four priority areas, the action plan recognises the importance of monitoring and evaluation by the AHPPC Governance Group and through the national blood-borne virus (BBV) and STI strategies. Monitoring and evaluation plans for the new 2018 to 2022 strategies will be developed in consultation with state and territory governments and partners.
Implementation of Syphilis Action Plan
All health services and staff have an important role to play with regard to implementing the priority areas of the syphilis action plan. For an effective response, multifaceted approaches across services and regions that focus on the four priority areas are needed. Health services and staff should consider how they can contribute to ensuring those priority areas are implemented or enhanced. Responses could include the following:
- increase awareness of the outbreak in the community, particularly with regard to who is affected, the importance of early detection and treatment, and the prevention of congenital syphilis
- increase awareness among women and antenatal services of the risk and prevention of congenital syphilis and the importance of staying connected with health services early and throughout the pregnancy
- use the skills of Aboriginal health and community workers and appropriate women in the community, such as Elders and grandmothers, to assist and support young pregnant women to engage with early and regular antenatal care
- facilitate community engagement and awareness through meetings with community Elders and leaders, boards of health services and community organisations; organise community meetings; use local radio, social and print media to provide information
- provide or facilitate access to training to ensure the workforce at primary care, antenatal services and hospitals are familiar with the updated CDNA guidelines, particularly with regard to the increased frequency of testing and urgency of treatment
- provide orientation to new and locum staff regarding the syphilis outbreak, testing and management guidelines, notifications and the role of regional public health units (PHUs)
- use the regional PHUs to provide or facilitate training and assist with community education and awareness.
Notification of syphilis and the role of PHUs in WA
In WA syphilis is notifiable under the Public Health Act 2016 and the Public Health Regulations 2017. A notification form needs to be completed by a medical officer or nurse practitioner and faxed to the nearest regional or metropolitan PHU as soon as possible and within 72 hours of the diagnosis. The receipt of a notification form will trigger the unit to contact the service provider to complete an enhanced surveillance form and discuss treatment and contact tracing.
Laboratories are also required to report test results that indicate a likely new infectious syphilis case. Notifications are stored on the WA Notifiable Infectious Diseases Database (WANIDD), access to which is restricted to disease control medical officers and nurses at the Communicable Disease Control Directorate (CDCD) and regional PHUs. PHU staff check new notifications on WANIDD daily, and prioritise and discuss any new syphilis notifications with the Medical Officer to verify the case and treatment required. Identifying a new case on WANIDD will also trigger a phone call from the PHU to the relevant service provider. As laboratories report on test results only, they may miss early cases of infectious syphilis. PHUs therefore also rely on clinicians to notify them on the basis of clinical findings to trigger a response and particularly to ensure early cases are not missed.
Syphilis: testing and treatment
Detailed protocols regarding syphilis testing and clinical management are available in the Silver Book and the Australian STI Management Guidelines. While not replicating those protocols or providing details about treatment regimens, the following information aims to highlight some of the key information regarding the natural history, testing and management of syphilis.
Clinical stages of syphilis
Syphilis (Treponema pallidum) is associated with different clinical stages although about 50 per cent of people infected have no symptoms.
Primary syphilis: A sore (or chancre) may occur at the site of infection, nine to 90 days after transmission. Chancres are typically painless, 1 to 2 cm in diameter, single or a few sores (on opposed skin) with associated lymphadenopathy. Chancres heal rapidly with treatment; without treatment they will heal spontaneously in three to eight weeks and may still be present in up to one-third of people at the onset of secondary syphilis symptoms.
Secondary syphilis: Untreated, syphilis enters a secondary stage marked by a range of signs and symptoms that can come and go over 12 months. Symptoms resolve rapidly with treatment; and spontaneously without treatment within two years and can include any of the following:
- sores or lumps on mucosal membranes (condylomata lata)
- systemic symptoms such as low-grade fever, malaise, headache, muscle aches and pains, lymphadenopathy
- rashes on palms and soles, maculopapular rash on the body
- patchy hair loss of the scalp and eyebrows.
Latent syphilis: Occurs after the resolution of secondary symptoms, when signs and symptoms are no longer present but the infection remains latent and detectable in the blood. While most sexual transmission occurs during primary and secondary syphilis in the presence of infectious sores, transmission from mother to baby can occur during pregnancy via blood up to nine years after the initial infection. Treatment of latent syphilis differs, depending on whether it was acquired within the past two years (early latent) or more than two years ago (late latent syphilis).
Tertiary syphilis: Can cause bony, cardiovascular and neurological changes in up to one-third of untreated people at least seven years after the initial infection but is now rare due to effective treatment and the widespread use of antibiotics.
Congenital syphilis: Syphilis can be transmitted from mother to baby during pregnancy and at delivery. Transmission is extremely high in early syphilis (90 to 100 per cent transmission in primary or secondary) and decreases over time but can still occur up to nine years after the initial infection. The outcome of syphilis in pregnancy depends on what stage the mother was infected and therefore at what stage in pregnancy it is transmitted. Poor outcomes include mid-term miscarriage, death in utero, stillbirth and congenital syphilis. Congenital syphilis refers to a range of abnormalities and manifestations that may or may not be evident at birth. Babies infected in late pregnancy or delivery may have no clinical abnormalities evident at birth but will likely present with congenital syphilis within the first few years of life if not managed appropriately at birth.
The diagnoses of tertiary and congenital syphilis are difficult and should always be done in consultation with an appropriate specialist.
Who and when to test for syphilis
Prompt and appropriate testing and management of syphilis is essential to:
- prevent the ongoing transmission to sexual partners
- prevent transmission from mother to baby and subsequent poor outcomes such as miscarriage, stillbirth and congenital syphilis
- reduce transmission of HIV and other STIs and BBVs, which increase in the presence of genital sores.
In the context of the current syphilis outbreak, practitioners should maintain a low threshold for testing and treating people presenting with any signs or symptoms that could be due to syphilis or other STIs and BBVs. In addition, the frequency of screening should increase among those at highest risk, in particular pregnant women, 15 to 30 year olds and MSM. Testing for syphilis should always be included when conducting a thorough check-up for STIs and BBVs and when any other STI or BBV has been detected, as co-infections are common.
Test for syphilis when someone of any age presents with any signs and symptoms possibly due to syphilis, other STIs and BBVs such as:
- genital ulcers, sores or lumps
- rashes in genital skin
- unexplained rashes anywhere on the body
- patchy hair loss in the scalp or eyebrows
- unexplained headache, fevers, muscle aches pains or lymphadenopathy
Or when any STI or BBV is detected.
Asymptomatic screening for syphilis should be done routinely in the following circumstances:
- Pregnancy:
- all women at first visit
- repeat at 28, 36 weeks, delivery and 6 weeks post-partum if syphilis is detected or treated during pregnancy and for all high-risk women, including all women living in the Goldfields, Kimberley, Midwest and Pilbara
- Thorough check-up for STIs and BBVs including:
- at least annually for all 15 to 30 year olds and three to six monthly if casual partners
- new or change of partner
- at follow-up when any STI or BBV is detected, if not tested at the initial presentation
- if a contact of a person with any STI or BBV
- if requests a sexual health check-up
- at adult health checks for 15 to 30 year olds (up to 40 years, depending on local epidemiology)
- MSM at least annually, and three to six monthly with casual partners
- HIV positive up to four times a year with a routine CD4 cell count and viral load testing.
Men and non-pregnant women treated for infectious syphilis should have a follow-up clinical assessment and repeat rapid plasma reagin (RPR) taken at three, six and 12 months. Note that the RPR is used to monitor response to treatment. Once reactive, the syphilis screening test will remain positive for life and does not need to be repeated.
Women treated for syphilis during pregnancy should at a minimum be retested in the third trimester, at delivery and six weeks post-partum; however, management may vary depending on when syphilis was acquired, and should always be done in consultation with the regional PHU and appropriate specialists.
While it is important to increase the frequency of testing for syphilis among people at highest risk, asymptomatic screening at a population level among people over the age of 40 years should be avoided. Be mindful that in many remote areas where syphilis has been endemic in the past, a significant proportion of people over the age of 40 years will have evidence of exposure to syphilis in the past on their screening test, as the test will remain positive for life, regardless of treatment. *
Most people aged over 40 with reactive syphilis serology will have a history of being treated in the past and are therefore not at risk of transmitting syphilis or developing tertiary syphilis. While there may be individuals in that age group who remain at risk of STIs and should be tested appropriately, population screening of that age group has little benefit with regard to case detection but could consume a significant amount of time and resources at the expense of directing appropriate case detection and management to those at highest risk. Remember, the majority of cases of infectious syphilis among Aboriginal people are among 15 to 29 year olds with 15 to 19 year old women being the highest risk age group. Resources to increase case detection should remain focused on those groups at higher risk and not be diverted to asymptomatic screening among low prevalence age or population groups.
* Clinical audits conducted in WA between 2008 and 2013 identified syphilis sero-prevalence, indicating past exposure, of greater than 30 per cent among people aged older than 40 years living in the Pilbara, Goldfields and Kimberley areas of WA.
How to interpret syphilis test results
Interpreting syphilis test results can be difficult, particularly without the availability of previous test results and treatment histories. A key role of PHUs is to assist with the accurate interpretation of syphilis serology by having access to and managing a central register of information regarding previous test results and treatments that may have been generated from different health services.
In order to interpret syphilis test results you need to know the:
- treponemal test result, and
- RPR test result, and
- previous syphilis serology results, and
- history of treatment.
Treponemal tests detect specific treponemal antibodies and are used as a screening test to identify whether someone has been exposed to syphilis or not. Most laboratories currently use a treponemal test that is reported as reactive or non-reactive. Other specific tests include enzyme immunoassay (EIA) immunoglobulin M (IgM) and immunoglobulin G (IgG), treponema pallidum haemagglutination assay (TPHA), treponema pallidum particle agglutination assay (TPPA), fluorescent treponemal antibody absorption (FTA Abs) as well as the newer POCT.
A non-reactive test indicates that the person has never been exposed to syphilis; however, it should be repeated in two weeks, if exposure to infection was very recent.
A reactive test:
- indicates the person has been infected with syphilis
- does not tell you:
- how long ago the person was infected, or
- whether they have been treated in the past, or
- whether they currently require treatment.
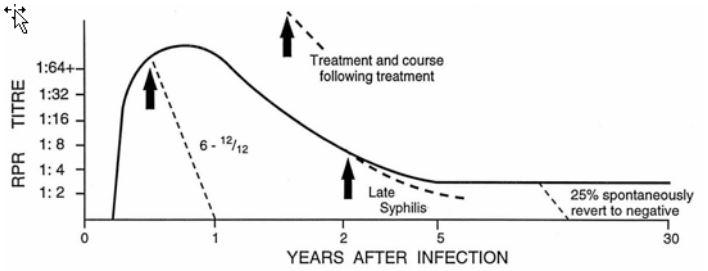
Non-treponemal tests detect non-specific antibodies. The RPR is the most common non-treponemal test in use and is done by the laboratory if the treponemal (screening) test is reactive. The RPR is performed manually. Reactivity is measured by serial dilutions and is reported as a 'titre'. The RPR titre changes over the course of an infection and in response to treatment . While an RPR does not tell you whether someone has been treated, it can give some indication of infectivity and is used to monitor treatment and identify reinfections.
- A two titre or fourfold fall in the RPR (e.g. 1:32 to 1:8) within six months following treatment of infectious syphilis usually indicates an adequate response to treatment.
- The RPR is unlikely to fall if the baseline titre is very low (as in latent syphilis) and therefore cannot be used in this context to monitor treatment response, but it can be used to identify new infections.
- A two titre or fourfold rise from a previous RPR result (e.g. 1:2 to 1:8) can indicate a new infection.
Venereal disease research laboratory (VDRL) test is a non-treponemal test which is currently only used in Australia for testing cerebrospinal fluid (CSF).
Syphilis nucleic acid amplification test (NAAT/PCR)
A swab should be taken for the syphilis NAAT/PCR test directly from any sore or lesion possibly due to primary or secondary syphilis. A reactive NAAT/PCR test from a lesion confirms infectious syphilis. Indicate on the pathology form where the swab has been taken from (e.g. genital ulcer) and request 'syphilis and herpes PCR'. A blood test should always be taken at the same time for screening and RPR testing if infectious syphilis is suspected.
NOTE: Blood tests for syphilis provide valuable information and a baseline against which to measure future testing, response to treatment and reinfections. Blood tests should always be taken if syphilis is suspected and an RPR taken again at the time of commencement of treatment to provide a baseline against which to measure response to treatment. If a point of care test has been conducted and is reactive, venous blood must also be sent to the laboratory for RPR as outlined. The lack of regular transportation to the laboratory is not a reason not to take blood tests. Check specific storage and transportation requirements with the local laboratory but, in general, specimens can be kept in the fridge and should be transported at 2 to 8°C.
False positive test results are uncommon but can occur with both treponemal and RPR tests. False positive treponemal tests may be identified in the laboratory as an equivocal or indeterminate test result but confirmatory tests are usually conducted with another treponemal test before the result is reported as reactive or non-reactive.
The RPR test is read manually and therefore results may vary slightly among specimens taken at different times or processed at different laboratories. Biological false positive results can also occur with the RPR for a number of reasons, including acute infections, injecting drug use and pregnancy. False positive RPR results should only cause a low titre reading (1:1, 1:2) while laboratory errors or variations are generally only within one titre of each other. Reactive RPR results should always be considered as true positives among people at risk and an increase in RPR of two titres from the previous RPR considered a likely new infection.
False negative test results can occur among people who have:
- very early syphilis and are tested before the test is measurable in the blood
- a 'prozone reaction' whereby a large antibody response can make the test inaccurate
- immune suppression due to HIV or other causes.
If there are any concerns about possible false positive results among people at low risk of infection, or false negative results among people likely to have syphilis, always contact the regional PHU or appropriate specialists for advice and repeat testing.
Graph 3. Variation in RPR results over time and with treatment
Syphilis POC tests
The Determine Syphilis TP is currently the only POC test registered for use in Australia and is being rolled out in response to the syphilis outbreak. The Determine Syphilis TP is a treponemal test that can be used with whole-blood samples from either finger-prick or venepuncture. As with other treponemal tests, a reactive test indicates exposure only, and in isolation of other tests and treatment histories, does not provide any information about when the infection was likely acquired or whether the person has been treated in the past or not. If a POC test is done at the bedside and is reactive, blood must be sent to the laboratory for RPR testing and all test results whether reactive or non-reactive need to be appropriately documented within the client's medical records and forwarded to the regional PHU. In settings where POC tests will be used, staff need to be appropriately trained in order to conduct the test, interpret results and relay test results accurately to the client. Staff should be provided with POC test user manuals, ensure quality assurance is conducted and comply with certification, surveillance, monitoring and notification requirements. As the roll out of POCT for syphilis is recent, information may change. Check with your local PHU or the Sexual Health and Blood-borne Virus Program (SHBBVP) for updated information.
Syphilis POC tests can be a useful addition to laboratory testing and can lead to a reduction in the time interval between testing and treatment. However, they also have limitations that must be taken into account when being used:
- The Determine Syphilis POC test currently in use provides an adjunct to, but does not replace, syphilis tests conducted in the laboratory:
- If a POC test is non-reactive, venous blood does not need to be sent to the laboratory for syphilis screening unless there is concern about very recently acquired syphilis or symptoms suggestive of syphilis.
- If a POC test is reactive, venous blood does need to be sent to the laboratory for RPR.
- The syphilis POC test is a treponemal test and a reactive test result indicates exposure only.
- A reactive POC test does not indicate when the person was infected, if they have been treated or if they require treatment.
- As with other treponemal tests, once reactive it will remain reactive for life and should not be repeated.
- Indications for use:
- A POC test should only be used on people who have never been tested or who have never had a reactive treponemal or screening test.
- To be cost-effective, its use should be limited and directed to those at highest risk of syphilis – antenatal women, 15 to 30 year olds, MSM and individuals at high risk.
- Limitations to use:
- It should not be used on people who have ever had a reactive treponemal test as it will return a reactive result; therefore, it has no value in this context.
- If reactive, venous blood is still required to be sent to the laboratory for RPR testing.
- In remote areas with previous endemic syphilis, a significant number of people aged over 40 years will return a reactive result. Most will have been adequately treated in the past.*
- Inappropriate use can lead to over-treatment of people, which is not only a waste of time and resources but has the potential to cause unnecessary damage to relationships and domestic violence.
- Both reactive and non-reactive test results need to be recorded in the client's medical record and relayed to the regional PHU syphilis register.
Before using a syphilis POC test, check the client's previous syphilis testing history in their medical records:
- If a syphilis screening test has ever been reactive, the POC test will also be reactive and therefore should not be used – send venous blood to the laboratory for RPR.
- If a client's last documented syphilis screening test was non-reactive, a reactive POC test indicates a new infection acquired since the last non-reactive screening test – commence treatment as a new infection and send venous blood to the laboratory for RPR.
- If there is no previous testing history and the POC test is reactive, this indicates they have been infected with syphilis but does not tell you when:
- contact the PHU to check if the patient has ever had a previous screening test and treatment
- commence treatment on the spot if they have any symptoms, are a contact or are at high risk of syphilis.
New infection
Remember that if a POC test or clinical signs and symptoms identify a likely new infection:
- Take venous blood and send it to the laboratory for RPR.
- Commence treatment.
- Take a full sexual history.
- Conduct an examination as appropriate.
- Test for other STIs and BBVs.
- Initiate contract tracing.
- Advise the client to abstain from sex until five days after contact(s) have been treated.
- Complete a notification form and fax it to the regional PHU.
- Contact the PHU for advice.
Recommendations for the clinical management of syphilis
To improve the clinical management of infectious syphilis, the CDNA National Syphilis Guidelines emphasise the importance of prompt and appropriate management of cases and contacts that support the existing state and national STI management guidelines. They include the following recommendations:
- Pregnant women at high risk or living in outbreak areas should be tested for syphilis up to five times during their pregnancy (first visit, 28 weeks, 36 weeks, delivery and six weeks post-partum).
- Infectious syphilis in a pregnant woman requires an urgent response, with treatment and follow-up commenced as soon as possible and within 24 hours.
- Treatment should be given at the time of presentation to people presenting with signs or symptoms of primary or secondary syphilis.
- Treatment of infectious syphilis identified on serology should be given as soon as possible and ideally within two days.
- An RPR test (a simple blood test that screens for syphilis) should be taken at baseline on the day of treatment and repeated between three and six months later and 12 months following treatment, ideally using the same laboratory.
Contact tracing
In the context of the syphilis outbreak, contact tracing of infectious syphilis cases, and particularly those involving pregnant women, should be managed urgently and as a priority. When conducting contact tracing of infectious syphilis cases among men, always ask up front if their contact(s) are or could be pregnant and explain the importance of treating pregnant women urgently. While some cases may involve significant time and human resources to ensure all contacts are treated appropriately and in a timely manner, the importance of doing so should be stressed in order to prevent ongoing transmission, congenital syphilis and neonatal deaths. Pregnant women with syphilis need to be informed about the risk of transmission to their baby, treatment, the need for ongoing monitoring and the high risk of reinfection later in pregnancy if their sexual partner(s) are not treated promptly and appropriately. Women should be advised to abstain from sex until five days after their regular partner(s) are treated, or until any symptoms have resolved (whichever is the longer).